The Lower Limbs are specialized for transmission of body weight and locomotion. A simple description of comparative anatomy of limbs vastly eases the understanding of their structure and function.
Parts/Regions
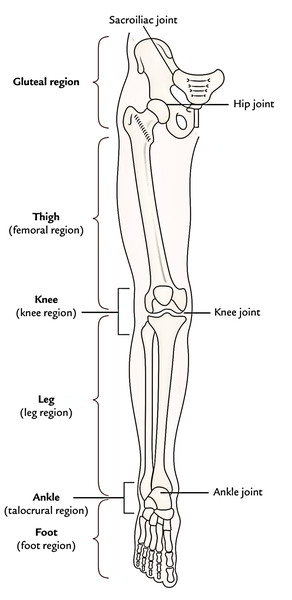
For illustrative purposes, the lower limb is split into 6 parts or regions:
- Gluteal region.
- Thigh or femoral region.
- Knee or knee region.
- Leg or leg region.
- Ankle or talocrural region.
- Foot or foot region.

Gluteal Region
The gluteal region is located on the back and side of the pelvis. It is composed of 2 parts: the rounded notable posterior region referred to as buttock and lateral less notable region referred to as hip or hip region.
The buttock is bounded superiorly by the iliac crest, medially by the intergluteal cleft, and inferiorly by the gluteal fold. The majority of it creates the gluteal muscles. The hip region overlies the hip joint and greater trochanter of the femur.
Thigh or Femoral Region
The femoral region is located between the gluteal, abdominal, and perineal regions proximally and the knee region distally. The bone of the thigh is femur, which articulates with the hip bone in the hip joint and upper end of the tibia and patella in the knee joint.
The abdomen is demarcated from the thigh anteriorly by the inguinal ligament and medially by the ischiopubic ramus. This junction between the abdomen and thigh is named inguinal region or groin. The gluteal fold is the upper limit of the thigh posteriorly. The lower part of the back of thigh and back of the knee is referred to as ham (L. poples).
Knee or Knee Region
The knee region consists of bulges (condyles) of the femur and tibia, head of fibula, and patella (knee cap). The patella is located in front of the distal end of femur and medial and lateral femorotibial joints. The posterior aspect of the knee presents a well defined hollow termed popliteal fossa.
Leg or Leg Region
The leg region is located between the knee and ankle regions. The leg includes 2 bones: a long and thick medial bone- the tibia, and long and narrow lateral bone- the fibula. The bulge on the posterior aspect of the leg created by a large triceps surae muscle is referred to as calf (L. sura).
Ankle or Talocrural Region
The ankle region contains distal part of the leg, and bulges (malleoli) of tibia and fibula. The ankle joint can be found between the malleoli and the talus.
Foot or Foot Region
- The foot is the distal part of the lower limb. It includes 7 tarsals, 5 metatarsals, and 14 toe bones (phalanges). The superior outermost layer of the foot is referred to as dorsum of the foot and its inferior surface is known as the sole of the foot. The sole is homologous with the palm of the hand. The foot gives a stage for supporting the body weight when standing and plays a key function in locomotion.
- The foot has gotten maximum changes during development. In the lower primates (example, apes and monkeys), it’s a prehensile organ and grab the boughs with their feet. They can oppose their great toes over the smaller toes. In individuals, the great toe comes to is located in keeping with other toes and loses its power of opposition. It’s considerably enlarged to supply primary support to the body. Its 4 smaller toes due to reduction of prehensile function have become vestigial and reduced in size. The tarsal bones have gotten large, powerful, and wedge-shaped to give stable support.
- The 4 major parts of the lower limb are summarised in Table below. The basic structure of the lower limb is quite similar to that of upper limb, but it’s changed to support the weight of the body and for locomotion.
- The lower limb joins the pelvic girdle in the hip joint. This girdle is composed of the 2 hip bones which join anteriorly at the pubic symphysis and posteriorly with the sacrum in the sacroiliac joints. The lower limb is supported by the heavy bones. The femur (largest and strongest bone of the body) articulates superiorly with the pelvis in the hip joint and inferiorly with the upper end of tibia in the knee joint. The tibia and fibula joint with every other at proximal, intermediate, and inferior tibiofibular joints. The distal ends of these bones articulate together with the talus to create the ankle joint.
| Parts | Bones | Joints |
|---|---|---|
| Gluteal region (on side and back of pelvis) | Hip bone | Sacroiliac joint |
| Thigh (from hipto knee) | Femur | 1. Hip joint 2. Knee joint |
| Leg (from kneeto ankle) | 1. Tibia 2. Fibula | 1. Tibiofibular joints 2. Ankle joint |
| Foot (from heelto toes) | 1. Tarsals (7) 2. Metatarsals (5) 3. Phalanges (14) | 1. Intertarsal joints(e.g., subtalar talocalcaneonavicular, transverse tarsal, etc.) 2. Intermetatarsal joints 3. Metatarsophalangeal joints 4. Interphalangeal joints |
Bones
Each lower limb contains 31 bones:
- Hip bone/innominate bone the bone of gluteal region (1).
- Femur, the bone of thigh (1).
- Patella or knee cap (1).
- Tibia and fibula, the bones of leg (2).
- Tarsal bones (7).
- Metatarsals (5)
- Phalanges, (14).
Femur
The femur, or thigh bone, is the largest and strongest bone of the body. Structures at the proximal end include the rounded head, a short neck, and two large processes that are sites of muscle attachment: a superior, lateral greater trochanter (tro-kan’-ter) and an inferior, medial lesser trochanter. The head of the femur fits into the acetabulum of the coxal bone. The neck is a common site of fractures in older people. At the enlarged distal end are the fateral and medial condyles, surfaces that articulate with the tibia.
Patella
The patella, or kneecap, is located anterior to the knee joint. It is embedded in the tendon of the quadriceps femoris, which extends over the anterior of the knee to insert on the tibia. The patella offers protection to the structures within the knee joint during movement.
Tibia
The tibia, or shinbone, is the larger of the two bones of the leg. It bears the weight of the body. Its enlarged proximal portion consists of the fateral and medial condyles, which articulate with the femur to form the knee joint. The tibial tuberosity, a roughened area on the anterior surface just distal to the condyles, is the attachment site for the patellar ligament. The distal end of the tibia articulates with the talus, a tarsal bone, and laterally with the fibula. The medial malleolus (mah-le-o ‘-lus) forms the medial prominence of the ankle.
Fibula
The fibula is the slender, lateral bone in the leg. Both ends of the bone are enlarged. The proximal head articulates with the lateral surface of the tibia but is not involved in forming the knee joint. The distal end articulates with the tibia and talus. The lateral malleolus forms the lateral prominence of the ankle.
Tarsal Bones, Metatarsals, and Phalanges
The skeleton of the foot consists of the tarsal bones (ankle), metatarsals (instep), and phalanges (toes). Seven bones compose the tarsal bones. The most prominent tarsal bones are the talus, which articulates with the tibia and fibula, and the calcaneus (kal-ka’n-e-us), or heel bone. Five metatarsals support the instep. They are numbered I to V, starting with the metatarsal adjacent to the great toe. The tarsal bones and metatarsals are bound together by ligaments to form strong, resilient arches of the foot. Each toe consists of three phalanges (proximal, middle, and distal), except for the great toe, which has only two (proximal and distal).
Transmission of The Body Weight via Lower Limb
The body weight is transferred from the vertebral column via sacroiliac joints to the pelvic girdle and from pelvic girdle via the hip joints to the femurs.
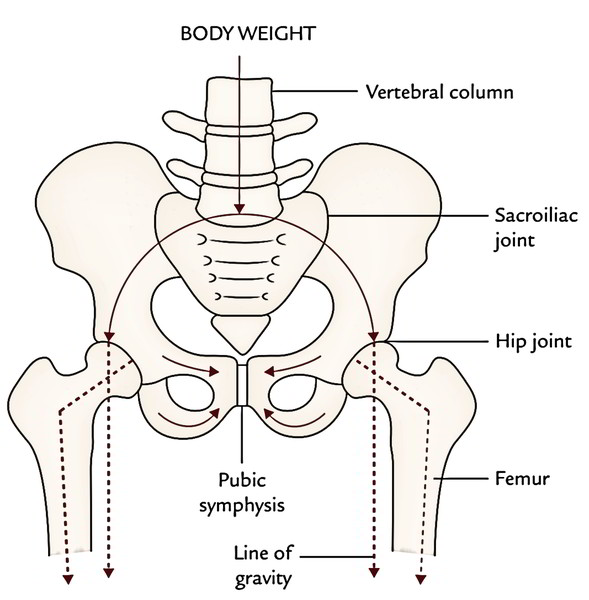
To support the erect position economically, the femurs are oblique being directed inferomedially inside the thighs so that during standing the knees are close to every other and put directly below the trunk. As a consequence, the centre of gravity falls to the vertical lines of the supporting legs and feet.
A little description of comparative anatomy is likely to allow it to be effortless to understand. In quadrupeds, the femurs are vertical and knees are apart with trunk suspended between the limbs.
- The body weight is transferred from the knee joint to the ankle joint by the tibia. The fibula doesn’t joint together with the femur, thus will not transfer any weight. At the ankle, the weight carried by the tibia is transformed to the talus- the keystone of the longitudinal arch of the foot. The longitudinal arch created by the tarsals and metatarsals, equally distribute the weight between the heel and foot when standing. In this manner the foot gives a flexible but stable stage to support the body. The weight bearing points of the foot are medial process of the calcaneus posteriorly and 6 identical Pillars anteriorly created by the heads of 4 lateral metatarsals and 2 sesamoid bones (1 on every side of V-shaped ridge) below the head of first metatarsal.
Manner of Weight Distribution to The Feet
The body weight of a man weighing say 48 kg when standing (in essential position) is doled out as follows:
- 24 kg goes to every lower limb.
- In every limb, 12 kg goes to the medial process of calcaneus and 12 kg to the metatarsals.
- The metatarsals present 6 points of equivalent contact with all the earth, viz., heads of lateral 4 metatarsals and 2 sesamoid bones below the head of first metatarsal every supporting 2 kg. Therefore, the great toe supports the double load of body weight in comparison with the other toes of the foot.
The line of gravity of the body goes through the cervical vertebrae, anterior to the thoracic vertebrae, via the lumbar vertebrae, anterior to the sacrum, posterior to the hip joints, and anterior to the knee and ankle joints.
Muscles
- The muscles of the lower limb are powerful and movements generated by them are rough than those created by the muscles of the upper limb.
- The major muscles in the gluteal region are gluteus maximus, gluteus medius, and gluteus minimus. The gluteal muscles primarily rotate the thigh laterally.
- In the thigh and leg, the deep fascia creates intermuscular septa and break up these regions into underlying compartments. The thigh is split into anterior, medial, and posterior compartments. The muscles in the anterior compartment are mainly extensor of the knee joint. The primary muscle in this compartment is quadriceps femoris, which is composed of 4 parts: vastus lateralis, vastus medialis, vastus intermedius, and rectus femoris. The muscles of medial compartment of the thigh are adductors of the hip joint. The muscles of posterior compartment of the thigh are termed hamstring muscles. They’re extensors of the hip joint and flexors of the knee joint.
- The leg is split into anterior, lateral, and posterior compartments. The muscles of the anterior compartment are chiefly dorsiflexors of the ankle and extensors of the toes. The muscles of lateral compartment plantarflex and evert the foot. The muscles of posterior compartment are split into superficial and deep groups by transverse fascia of the leg. The superficial muscles, example, gastrocnemius, and soleus, which jointly create the triceps surae that is added by a long thick tendon (tendoachillis) into calcaneus. They act on calcaneus to plantarflex the foot. The muscles of deep group bend the toes and plantarflex the ankle.
- The foot has 20 individual muscles, out of which 18 are situated in the sole and only 2 are situated on the dorsum of the foot. The muscles of the sole are ordered into 4 complex layers. Despite their layered arrangement, the muscles of lone function mainly as a group during the support period of the posture, keeping the arches of the foot.
- The antigravity muscles of the lower limb are much better developed than those of the upper limb only because they lift up the entire body to reach the erect bearing and in walking up the stairs. These muscles are: gluteus maximus (extensor of the hip), quadriceps femoris (extensor of the knee), and gastrocnemius, and soleus (plantarflexors of the ankle). They’ve extensive origin and bulky muscle abdomen.
Clinical Significance
Intramuscular injection: The muscles typically utilised for intramuscular injection in the lower limb are: (a) gluteus medius of gluteal region in adults (most common site) and (b) vastus lateralis muscle of the thigh region in kids.
Nerves
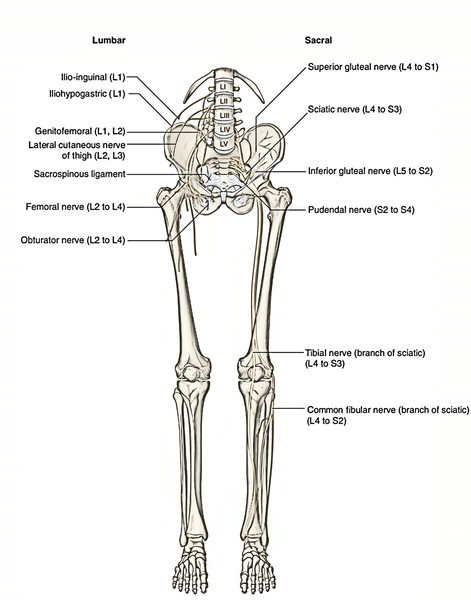
- The nerves of the lower limb are originated from lumbar plexusof nerves (L1 L4) inside the posterior abdominal wall andsacral plexus of nerves (L4 S4) in the posterior pelvic wall.
The nerves of the lower limb are: femoral, obturator, sciatic, tibial, and common peroneal nerves.
- Femoral nerve: It’s present on the very front of the thigh and innervates the anterior thigh muscles.
- Obturator nerve: It’s present on the medial side of the thigh and innervates the adductors of the thigh.
- Sciatic nerve (largest and thickest nerve in the body): It’s present in the gluteal region and the back of the thigh. It supplies muscles on the back of the thigh. In the lower part of the back of thigh, it breaks up into tibial and common peroneal nerves.
- Tibial nerve: It’s present on the rear of the leg and supplies all the muscles on the rear of the leg. At the ankle, behind medial malleolus, it breaks up into medial and lateral plantar nerves, which collectively supply all the muscles of the sole.
- Common peroneal nerve: At the lateral side of the neck of fibula, it breaks up into the deep and superficial peroneal nerves. The deep peroneal nerve is within the anterior compartment of the leg and supplies all the anterior leg muscles.
The superficial peroneal nerve is present in the lateral compartment of the leg and supplies all the lateral leg muscles.
Along with the muscles, all the nerves (vide supra) also supply joints and offer cutaneous innervation to the lower limb.
Arteries
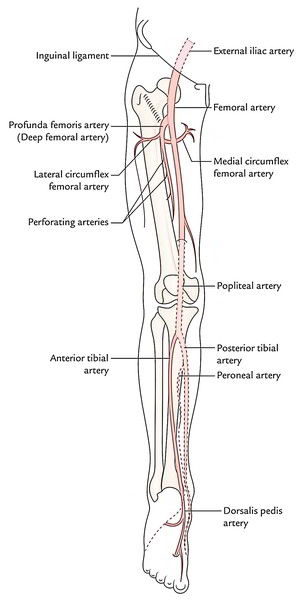
The blood to the lower limb is usually supplied by the femoral artery and its branches.
- Femoral artery: It starts at the midpoint of inguinal ligament as the continuance of the external iliac artery. It enters the front of thigh and immediately produces deep femoral artery (profunda femoris artery) which supplies all the structures of the thigh.
- Popliteal artery: It’s the continuance of femoral artery into the popliteal fossa. The popliteal artery descends via the popliteal fossa and in the head of fibula it breaks up into the anterior and posterior tibial arteries.
- Anterior tibial artery: It is located in the anterior compartment of the leg which it supplies and continues into the dorsum of the foot as dorsalis pedis artery.
- Dorsalis pedis artery: It is located on the dorsum of the foot which it supplies.
- Posterior tibial artery: It is located in the posterior compartment of the leg which it supplies. At the ankle, behind the medial malleolus it breaks up into medial and lateral plantar arteries.
- Medial and lateral plantar arteries: They’re the terminal branches of posterior tibial artery and supply the sole of the foot.
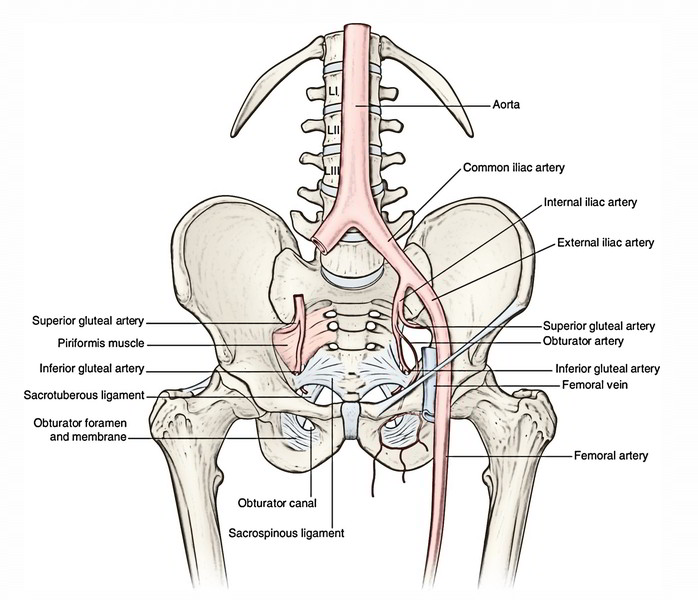
Along with the femoral artery the following arteries also give a little to the blood supply of the lower limb:
- Superior gluteal artery.
- Inferior gluteal artery.
- Obturator artery.
They’re all branches of the internal iliac artery.
Clinical Significance
Ssites where arterial pulse can be palpated/felt in the lower limb:
- Femoral pulse can be felt at the midinguinal point (i.e., the point midway to anterior superior iliac spine and pubic symphysis.
- Popliteal pulse can be felt behind the knee deep in the popliteal fossa with knee bent.
- Posterior tibial pulse can be felt behind the medial malleolus midway between it and tendocalcaneus.
- Dorsalis pedis pulse can be felt on the dorsum of the foot just medial to the tendon of extensor hallucis longus.
Acute arterial occlusion: It’s largely caused by embolism or thrombosis. It normally happens in the femoral artery where it produces the profunda femoris artery. The clinical features contain 5 P’s: Pain, Paresthesia, Pallor, Paralysis, and Pulselessness.
Chronic arterial occlusive disease: It’s largely caused by the atherosclerosis. It generally includes femoral or popliteal artery (50% of cases). Yet, in the diabetic patients, it could also include anterior tibial, posterior tibial, and peroneal arteries. Medically, it presents as intermittent claudication, i.e., deep leg pain in the leg on walking for some space that is alleviated by taking rest for 5-10 minutes and reoccurs on walking again for the same space.
Veins
The veins of the lower limb are classified into 3 types: superficial, perforating, and deep veins. The superficial veins convey with all the deep veins via perforating veins.
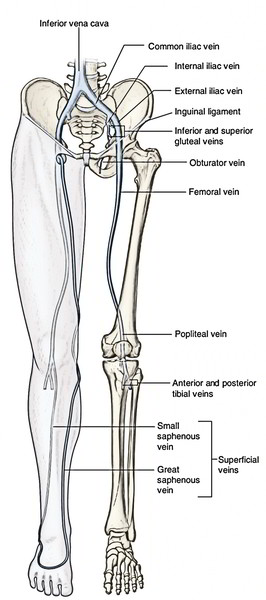
Deep Veins
They follow the arteries of the leg and eventually drain into femoral vein, which continues as external iliac vein. The termed deep veins are: venae comitantes of anterior and posterior tibial arteries, popliteal vein, and femoral vein. The deep veins are subject to muscle compaction (musculovenous pump) to ease the venous return.
Superficial Veins
They drain into deep veins via perforating veins. The called superficial veins are great and small saphenous veins, which starts from dorsal venous arch of the foot. The great saphenous vein ascends anterior to medial malleolus, continues along the medial side of leg and thigh before emptying into the femoral vein in the femoral triangle. The small saphenous vein ascends behind the lateral malleolus in the calf and empties into the popliteal vein in the popliteal fossa.
Perforating Veins (Perforators)
They attach and direct blood of superficial veins into the deep veins. The presence of valves in them keep the back flow from the deep veins.
The venous blood of the lower limb is emptied against gravity consequently, all the lower limb veins have valves to conquer the impact of gravity.
Clinical Significance
Varicose veins: The superficial veins (great and small saphenous veins) emptying skin always shunt their blood into the deep veins by perforating veins.
The incompetence of valves of perforating veins enables backflow of blood into superficial veins. This backflow causes dilatation of the superficial veins and their tributaries termed varicose veins.
Lymphatics
The lymphatics of the lower limb are classified into 2 types- superficial and deep.
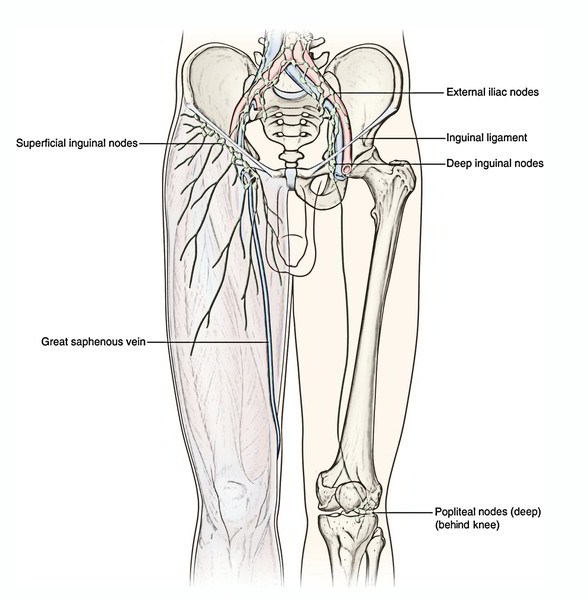
Superficial Lymphatics
They are located superficial to deep fascia and drain into the superficial inguinal lymph nodes present just below the inguinal ligament and near the terminal part of great saphenous vein. The lymph from buttock, perineum, and lower abdomen also drain into these lymph nodes.
Deep Lymphatics
They accompany the arteries and drain into deep inguinal lymph nodes present inside the femoral sheath, which in turn drain into iliac lymph nodes inside the pelvis and aortic lymph nodes in the lower posterior abdominal wall.
Lymph from glans penis/glans clitoris drain into deep inguinal lymph nodes located in the femoral canal that is called lymph node of Cloquet/ Rosenmuller.

 (53 votes, average: 4.66 out of 5)
(53 votes, average: 4.66 out of 5)