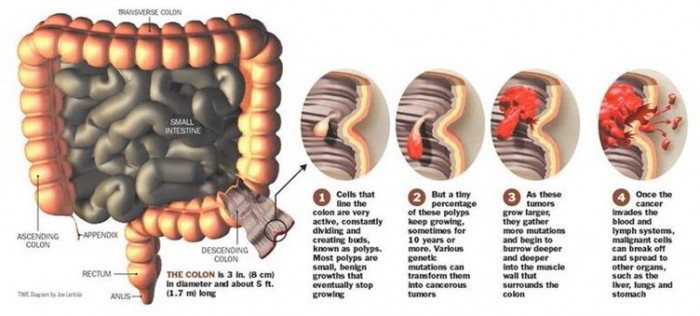
Malignant tumor of the colon and rectum. The colon is the large intestine, also called the large bowel. The rectum is a passageway linking the colon to the anus. Colorectal cancer is the third leading cause of all cancer deaths in America. An estimated 75 percent of the people that are diagnosed with colorectal cancer don’t have any family history of the disorder (although family and personal history should be thought to be a potential risk factor).
About 56,700 Americans die of colorectal cancer per year, and about 135,400 new cases are diagnosed yearly. In Canada, an estimated 6,400 people died of colorectal cancer in 2001, and 17,200 new cases of colorectal cancer were diagnosed.
Based on the National Center for Chronic Disease Prevention and Health Promotion, a department of the CENTERS FOR DISEASE CONTROL AND PREVENTION CDC), one third or more of all the colorectal departures in America could be prevented if everyone who was age 50 and older had regular screening tests for the disorder.
Sex and Race Variables
Although colorectal cancer has a high fatality rate, when considered in relation to the frequency of Diagnosis, colorectal cancer follows skin, prostate, and lung cancer for men. For girls, colorectal cancer Diagnosis follows skin, breast, and lung cancer in frequency of Diagnosis. Guys have a higher risk of colorectal cancer than girls do. African Americans have a significantly higher risk for colorectal cancer than Caucasians in America. Based on the National Cancer Institute, white men have a speed of 20.1 per 100,000, and black men have a greater rate of 27.2 per 100,000. White women have a speed of colorectal cancer of 13.7 per 100,000, compared to African American girls who confront a higher speed of 19.5 per 100,000.
Risks for Getting Colorectal Cancer
The risk for developing colorectal cancer increases with age. Other Risks for colorectal cancer include:
- Family or personal history of polyps
- Inflammatory bowel disease (ulcerative colitis and Crohn’s disease)
- Obesity
- Alcohol abuse
- Physical inactivity
Symptoms
An individual may have no symptoms in the early phases of colorectal cancer. When symptoms occur, the essential symptoms are:
- Blood in the stool
- A change in bowel habits
- Diarrhea or constipation
- Regular unexplained stomach cramping
- Unexplained weight loss
- Feces that are more narrow than is common for the individual
- Endured and unexplained tiredness
Other illnesses may also cause these nonspecific symptoms, and patients who experience them should see their physicians for an assessment.
Diagnostic Tools
There are several methods that physicians may diagnose colorectal cancer. The most straightforward technique is the digital rectal examination, where the physician inserts a lubricated finger in the rectum to feel for any abnormalities. This test may also detect prostate cancer in men. If any abnormalities are found, additional studies will be ordered.
Fecal Occult Blood Test
Additionally, there are lab tests for colorectal cancer, and the most frequently used test is the fecal occult blood test (FOBT). This test detects blood in the feces that cannot be seen by the person and may show colorectal cancer. People are given unique cards on which to gather their own little stool specimens. The lab will then assess the specimens on the cards for hidden (occult) blood.
Specialists recommend that individuals older than age 50 should have the FOBT annually. Sadly, based on the CDC, only about 21 percent of whites and African Americans have yearly FOBTs, and the percents of those having yearly FOBTs are even lower for Hispanic Americans (11 percent) and Asians/Pacific Islanders (10 percent). Based on the CDC, if the fecal occult blood test were done every a couple of years on individuals ages 50-80, it’d reduce the death rate from colorectal cancer. Nevertheless, it should be noted that too little occult blood will not definitively rule out colorectal cancer.
Based on gastroenterology medical professor and writer Anil Minocha, M.D., in his novel for medical residents, The Gastroenterology Resident Pocket Survival Guide, just 20-40 percent of patients who have colorectal cancer also have occult blood in their feces. Because of this, most individuals older than age 65 need additional testing, despite the effects of the FOBT.
Invasive Screening Processes
There are also several invasive processes to detect colorectal cancer, for instance, flexible sigmoidoscopy, the colonoscopy, and the barium enema.
These processes differ in how each one is performed and how much of the bowel can be scrutinized. Additionally they differ in the activities the surgeon may take, if any, should cancerous or precancerous growths be identified during the process.
The patient’s level of consciousness also changes. By way of example, with the flexible sigmoidoscopy (using a flexible range, which can go around turns in the lower one fourth of the bowel), the patient is generally aware during the process.
With a colonoscopy, a more extensive screening process at which physician visually inspects the whole colon, patients may be given “conscious sedation,” or sedating drugs which will make them fall asleep. As of 2001, Medicare covers the colonoscopy as a screening tool.
During the double-contrast barium enema, patients are completely aware. Patients are administered a barium dye that bathes and emphasizes the colon, making it opaque on X rays, and then air is introduced to give a double comparison and make the X ray view even clearer. (With an individual contrast barium enema, just the barium is used.)
The groundwork for both the colonoscopy and the barium enema is similar: patients will take specific oral medication that causes diarrhoea and clears out their fecal matters in advance so the bowel can be more readily analyzed during the process. The colon may also be “cleaned out” (emptied) prior to a sigmoidoscopy, but most physicians rely instead on a couple of enemas rather than on oral medicine.
The activities the physician can take as an outcome of the findings during the process are also determined by the kind of process. As an example, polyps (precancerous growths) can be found during a sigmoidoscopy, but they cannot be removed unless the colon was totally cleaned out beforehand. Additionally, if polyps are found during a sigmoidoscopy, the physician will order a colonoscopy so the whole colon can be assessed for polyps and they’re able to be removed. The premise is that if one part of the colon has polyps, then the remaining portion of the colon may also have polyps and should be assessed.
A colonoscopy is considered the best process for discovering polyps because the colonoscopy examines the entire large bowel and because the physician can remove any polyps that are discovered. Polyps may also be found with a barium process, but they cannot be removed. A colonoscopy would have to be ordered to reach that target, getting the patient through an added process. Additionally, smaller polyps may be missed during a barium enema.
If the physician needs to remove tissue to check for cancer (a biopsy), this process cannot be performed during a barium enema. The physician may, however, perform a biopsy during either a colonoscopy or sigmoidoscopy.
Note: Individuals who have precancerous polyps should be followed up even more closely than others should because polyps may recur.
Recommendations for Testing
With elderly adults, some specialists advocate either an annual fecal occult blood test, joined with a flexible sigmoidoscopy every five years or a colonoscopy every 10 years. If the double-contrast barium enema is used, it should be performed every five to a decade.
These processes may be needed more often if there are risk factors for disease of the colon or if the physician advocates thus. Yet, just about a third of adults older than age 50 in America have had either a sigmoidoscopy or a colonoscopy within the recommended time frame. The truth is, the CDC estimated that as of 1999, just about 44 percent of adults older than age 50 had ever had either process.
Colonoscopy Is Preferred By Some Pros
Some specialists consider that a colonoscopy is the preferable diagnostic screening tool in asymptomatic elderly adults. Actually, Anil Minocha, M.D., chief of gastroenterology at the Southern Illinois University School of Medicine in Springfield, Illinois, says that having a sigmoidoscopy to screen for cancer is comparable to having just one breast analyzed in a mammogram because the sigmoidoscopy simply can look at part of the bowel and so can overlook cancers beyond the range of the examination.
One study, which offers powerful support to this perspective, was reported in a 2000 issue of the New England Journal of Medicine. Researchers reported on more than 3,000 old male patients at Veterans Administration hospitals who’d had colonoscopies. They discovered precancerous states in almost half (47 percent) of the patients and cancer in about 1 percent. The researchers said, “Many of these neoplasms wouldn’t be found with sigmoidoscopy.” In addition they said, “Most of the patients with cancer (73.3 percent) were identified before there was nodal involvement or distal spread and were thus candidates for curative treatment.”
Because most physicians need to treat patients when they’re in the precancerous or early cancerous periods when they’ve a better prognosis, the colonoscopy is apparently the finest diagnostic instrument to reach that aim.
Staging of Cancer
When colorectal cancer is found, physicians “period” it with a biopsy, or a tissue sample. Staging means that physicians discover how advanced the cancer is and how quick it’s growing. Then they do a phase group.
With colorectal cancer and other types of cancer, physicians use a system called the “TNM” system, developed by the American Joint Committee on Cancer. This system enables a categorization of the tumour based on determinations for how advanced the tumour is, (the “T”), whether or not the tumour has spread to nearby lymph tissues (the “N”), and whether or not the cancer has metastasized to distant tissues (the “M”). As an example, T1 means the cancer is in its first phase. At the T1 stage, the cancer is also called carcinoma in situ or intramucosal carcinoma. There are additionally T2, T3, and T4 levels. When the cancer is considered at the T4 level, it’s spread through the colon and to nearby organs or tissues. There are three fundamental phases of “N” advice. NO means there isn’t any lymph participation, N1 means there are cancer cells that are in one to three lymph nodes, and N2 means that cancer is discovered in four or more lymph nodes.
As for “M” groups, there’s either no spread to distant tissues or organs (MO), or there’s distribute (Ml).
Once the TNM groups of the tumour are discovered, the phase group can be made. With colorectal cancer, there are five period groups, beginning with Phase 0 (zero), which is a period of early cancer discovered exclusively within the inner lining of the rectum or colon.
If the cancer is Phase I, this means more of the internal wall of the rectum or colon is affected by the cancer. This can be either Tl, NO, MO or T2, NO, MO.
With Phase n, the cancer has farther improved in the colon or rectum but hasn’t spread to lymph nodes. This can be either T3, NO, MO or T4, NO, MO.
In Stage III, the cancer has spread to lymph nodes but not to the remaining part of the body. This can be any period of T, Nl, MO or any T, N2, and MO.
In Stage IV, the most advanced phase, the cancer has spread to distant tissues, like the lungs or the liver. This is likewise qualified as any T, any N, and Ml.
Treatment of Colorectal Cancer
Operation
Operation is the only feasible treatment for colorectal cancer and is the mainstay. Other alternatives, including chemotherapy and radiation therapy, are considered adjunctive. Operation is frequently advocated even when the cancer has spread to the surrounding tissues and is improved, mainly to stop bleeding and prevent obstruction.
When operation is performed, physicians will remove all or part of the cancerous colon/rectum. Lymph nodes in the region are also removed. Generally, the colon’s function can be preserved through reconnections; yet, if this is impossible, the patient may want a temporary or permanent colostomy. This implies that the waste material will go straight into a tote that’s external to the body and that will be periodically emptied by the patient. This may be a temporary process if it’s needed to permit time for the colon to fix. In about 15 percent of cases, a permanent colostomy is needed.
Chemotherapy
Some patients receive chemotherapy for colorectal cancer. It’s usually only used in colon cancer if the cancer is improved but is frequently used in rectal cancer in the least phases.
Anticancer drugs are generally added intravenously or occasionally with a catheter. Some types of drugs are obtainable in pill form. During the course of chemotherapy, the patient may feel nauseous, tired, and dizzy, and the anticancer drugs may also cause baldness.
Radiation Therapy
Another adjunctive choice along with chemotherapy would be to irradiate the cancerous tissue. Radiation may be given through a medication accessible at a hospital or an outpatient facility. In some instances, radiation pellets may be internally added. Radiation therapy may cause loss of appetite, nausea, fatigue, and irritation at the site of the radiation.
Clinical Trials Another alternative for patients with colorectal cancer would be to join a clinical trial in which new drugs or other treatments are being examined. These drugs and treatments are only accessible clinical trials, and offer patients another option.
Questions To Ask The Doctor
Based on the National Cancer Institute and other specialists, patients diagnosed with colorectal cancer should ask their physician these questions:
- What’s my point of cancer?
- What treatments do you recommend?
- What kinds of other physicians do I should see? (Surgeon, medical oncologist, radiation oncologist, or other kind of physician)
- Will I need a colostomy? If so, will it be temporary or long-term?
- Will I need to go into the hospital for my treatment? If so, for how long?
- How will my regular activities be influenced by my treatment?
- what’ll occur if I do not have the recommended treatment?
- What side effects should I expect from the treatments?
- What are the potential treatments for the side effects of treatment?
Pain Control
If the cancer becomes advanced, many patients will want pain control treatment like narcotics. There’s little point in worrying about whether patients will become hooked when their lives are finishing, and there’s considerable point in relieving as much pain as possible. An exhaustive discussion regarding the dangers and advantages of narcotic pain management with a doctor may reduce any anxiety over dependency.

 (46 votes, average: 4.74 out of 5)
(46 votes, average: 4.74 out of 5)